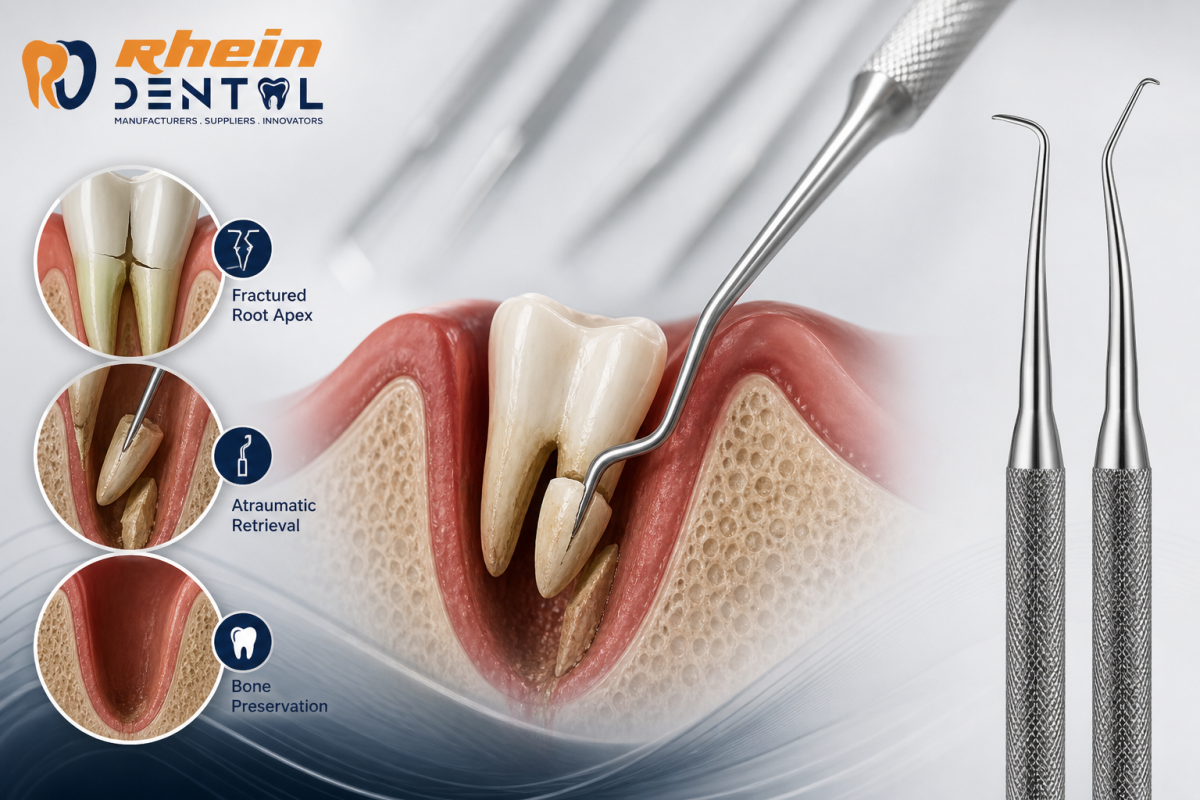
Fractured root apices are a common intraoperative challenge in exodontia—especially in endodontically treated teeth, brittle roots, or anatomically complex molars. The goal isn’t just retrieval; it’s doing so atraumatically, preserving surrounding bone and soft tissue for optimal healing and future prosthetic or implant considerations (Root pick tips and apical elevators techniques).
This guide breaks down how to use root tip picks and apical elevators effectively, with a strong focus on technique, control, and tissue preservation.
Why Root Tips Fracture in the First Place
Understanding the cause helps guide your retrieval strategy:
- Thin, curved, or divergent roots (common in maxillary molars)
- Sclerosed or brittle dentin (often in older patients)
- Excessive force during extraction
- Inadequate luxation before forceps use
- Hypercementosis or ankylosis
When a root tip fractures, avoid the instinct to “dig it out” aggressively. That’s where bone loss begins.
Instruments Overview
1. Root Tip Picks
Root tip picks are fine, sharp instruments designed to engage and tease out small root fragments.
Key features:
- Delicate, pointed working ends
- Angulated tips for access
- Minimal force application
Best used when:
- The fragment is visible or slightly subgingival
- There is a periodontal ligament (PDL) space to exploit
- Bone removal is not required
2. Apical Elevators
Apical elevators are more robust and provide controlled leverage in deeper or less accessible areas.
Key features:
- Thicker shanks for torque control
- Curved or straight working ends
- Designed for apical engagement
Best used when:
- The fragment is deeper in the socket
- Some resistance is present
- Controlled leverage is needed without removing bone
Core Principle: Preserve the Socket
The primary rule is simple:
Use the natural PDL space and socket anatomy instead of removing bone.
Every technique below revolves around this concept.
Step-by-Step Technique
Step 1: Visibility and Access
- Achieve adequate lighting and suction
- Reflect soft tissue gently if needed
- Avoid unnecessary flap elevation unless visibility is compromised
Step 2: Re-establish the PDL Space
Even after fracture, some PDL remnants exist.
- Use a periotome or fine elevator to re-enter the ligament space
- Work circumferentially with light apical pressure
- This step alone may loosen the fragment significantly
Step 3: Use the Root Tip Pick (First-Line Approach)
Technique:
- Insert the pick into the PDL space or alongside the fragment
- Engage the root surface—not the surrounding bone
- Apply gentle rotational or teasing movements, not prying
Important tips:
- Think “unlock,” not “force out”
- Avoid pushing apically (you may displace the fragment deeper)
- Maintain finger rest for precision
Step 4: Transition to Apical Elevator (If Needed)
If the fragment resists:
Technique:
- Insert the apical elevator into the PDL space
- Use controlled rotational leverage, not excessive force
- Support surrounding bone with your fingers
Key concept:
- Leverage should be directed along the path of least resistance, not against dense cortical bone
Step 5: Micro-Movement Strategy
Instead of one strong force:
- Apply small, repeated micro-movements
- Allow the ligament and socket to gradually expand
- This reduces the risk of bone fracture
Step 6: Delivery
Once mobile:
- Use suction, tweezers, or the pick to retrieve the fragment
- Avoid crushing delicate root tips
Advanced Tips to Avoid Bone Loss
✔ Use Apical Pressure Strategically
Apical pressure can help expand the socket slightly—but must be controlled and minimal.
✔ Avoid Blind Instrumentation
Never “hunt” for the root tip without clear direction. This causes unnecessary bone trauma.
✔ Respect Thin Cortical Plates
Especially in the maxilla, aggressive leverage can fracture buccal bone.
✔ Know When to Stop
If the fragment is:
- Very small
- Deeply embedded
- Close to vital structures (e.g., sinus or nerve)
…it may be safer to leave it in place if asymptomatic.
Common Mistakes to Avoid
- ❌ Using excessive force early
- ❌ Leveraging against bone instead of root
- ❌ Skipping PDL re-entry
- ❌ Driving the fragment deeper apically
- ❌ Immediate surgical removal without conservative attempts
When Surgical Intervention Is Needed
If conservative methods fail:
- Consider a minimal flap and bone troughing
- Use round burs with copious irrigation
- Remove only the necessary amount of bone
Even in surgical cases, the philosophy remains:
Minimal bone removal, maximum control.
Clinical Outcome Focus
Atraumatic retrieval ensures:
- Better socket preservation
- Reduced postoperative pain and swelling
- Improved healing
- Stronger foundation for implants or prosthetics
Final Thoughts
Mastering root tip picks and apical elevators isn’t about strength—it’s about precision, patience, and respect for anatomy. The difference between a traumatic and atraumatic extraction often comes down to how you handle those last few millimeters of root (Root pick tips and apical elevators techniques).
Slow down, feel the movement, and let the instrument do the work—not force.